

Arrhythmogenic Right Ventricular Cardiomyopathy
Definition

Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a primary disease of heart muscle that results in fibro-fatty replacement of the right ventricle, and the subepicardial region of the left ventricle. Patients are at high risk of ventricular tachyarrhythmias and sudden death.
Arrhythmogenic right ventricular cardiomyopathy (ARVC), biventricular, autopsy heart, young man who died suddenly playing basketball. Top left demonstrates increased fat in the outer walls of the right ventricle and left ventricular posterolateral walls. A higher magnification of the right ventricle is seen at top right; the anterior wall is nearly completely replaced with fat, and fibrofatty irregular posterior wall involvement is seen. Note that no actual thinning of the wall itself exists, although the muscular portion is in some areas completely missing. The bottom left demonstrates a full thickness of the right ventricle stained with Masson trichrome. The residual muscle is present only in a band-like area of scarring, and subepicardial scarring is present as well. The characteristic myocyte vacuolization, depicted at the bottom right, is seen in nearly all areas of ARVC within the scarred areas.
Epidemiology
The prevalence of ARVC has been estimated to vary from 1:2,500 to 1:5,000. In series of sudden cardiac death, it represents the cause of 2-5% of deaths in young adults, with higher incidences in exertional deaths and in certain regions of Europe.1
Etiology
The etiology of arrhythmogenic right ventricular cardiomyopathy (ARVC) is unknown. The presence of inflammatory infiltrates in most cases seen at autopsy has led to the theory that it is a resolving myocarditis.2 Families have been described with phenotypic alterations ranging from myocarditis to fibrofatty cardiac infiltrates, and imaging studies have demonstrated a progression from myocarditis to ARVC. More recently, genetic studies based on animal models, rare families with coincidental skin lesions, and, more recently, family studies of isolated cardiomyopathy have led to the discovery of mutations in genes related to the desmosome. ARVC may possibly be an inflammatory process that is modulated by genetic influences in desmosomal-related proteins.
Location
Although initially described in the right ventricle, microscopic examination of the heart in autopsy cases,3 or with sensitive imaging techniques,4 has established that most patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) have biventricular involvement. The left ventricular involvement is typical subepicardial and is probably similar in the right ventricle. However, because the right ventricle is relatively thin, the subepicardial nature of disease is difficult to appreciate in imaging studies and has only infrequently been investigated at autopsy.5
Clinical Features
The primary symptoms of arrhythmogenic right ventricular cardiomyopathy (ARVC) are related to arrhythmias and conduction disturbances.6 The pathologist is likely to encounter the disease at autopsy in cases of sudden death.1Approximately three-quarters of sudden deaths are exertional. ARVC is generally limited to the young, especially males under the age of 40, although the disease has been described up to the ninth decade.7 It is extremely uncommon under the age of 10 years.
Several clinical criteria for diagnosis have been proposed, including the Task Force of 2000,8 and a revision in 2002.9 Symptoms, hemodynamics, and ECG findings are relatively nonspecific, but advances in cardiac imaging, especially MR, have increased the reproducibility of clinical diagnosis.
Differential diagnosis
At autopsy, the major differential diagnoses include normal fat deposits in the right ventricle, and subepicardial scars of ischemic origin. Adipose tissue is normally present in the right ventricle, especially in the anterior wall toward the apex, but no associated fibrosis or myocyte changes exist. In the left ventricle, subepicardial scars can be associated with ischemic heart disease, especially if there is embolization of thromboembolic material from epicardial coronary lesions.
Several clinical criteria for diagnosis have been proposed, including the Task Force of 2000,8 and a revision in 2002.9 Symptoms, hemodynamics, and ECG findings are relatively nonspecific, but advances in cardiac imaging, especially MR, have increased the reproducibility of clinical diagnosis.
Differential diagnosis
At autopsy, the major differential diagnoses include normal fat deposits in the right ventricle, and subepicardial scars of ischemic origin. Adipose tissue is normally present in the right ventricle, especially in the anterior wall toward the apex, but no associated fibrosis or myocyte changes exist. In the left ventricle, subepicardial scars can be associated with ischemic heart disease, especially if there is embolization of thromboembolic material from epicardial coronary lesions.
Gross Findings
In cases of arrhythmogenic right ventricular cardiomyopathy (ARVC), the typical findings at autopsy include areas of thinning of the right ventricle, with fibrofatty change, in areas where fat is not normally found (outflow region, posterior wall). Pathologic findings at autopsy are wide ranging, depending on the stage and extent of the disease.
Some have postulated that ARVC begins in the right ventricle and progresses to biventricular involvement and heart failure. However, newer imaging techniques reveal that left ventricular involvement is typical from the onset.4 Autopsy studies from patients who die suddenly with the disease demonstrate biventricular involvement in most cases, with subepicardial left ventricular involvement and right ventricular fibrofatty infiltration. Left ventricular involvement grossly is that of scars in the subepicardial region, randomly throughout the ventricle; the fat is difficult to appreciate, and often the fibrosis is more conspicuous. The ventricular septum is relatively spared. Aneurysms of the right ventricle are present in only a minority of patients. Gross abnormalities are minimal, with the diagnosis made only microscopically.10
Some have postulated that ARVC begins in the right ventricle and progresses to biventricular involvement and heart failure. However, newer imaging techniques reveal that left ventricular involvement is typical from the onset.4 Autopsy studies from patients who die suddenly with the disease demonstrate biventricular involvement in most cases, with subepicardial left ventricular involvement and right ventricular fibrofatty infiltration. Left ventricular involvement grossly is that of scars in the subepicardial region, randomly throughout the ventricle; the fat is difficult to appreciate, and often the fibrosis is more conspicuous. The ventricular septum is relatively spared. Aneurysms of the right ventricle are present in only a minority of patients. Gross abnormalities are minimal, with the diagnosis made only microscopically.10
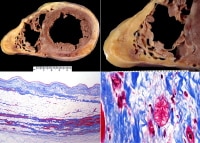
Gross findings at autopsy, ventricular arrhythmogenic right ventricular cardiomyopathy (ARVC). A suspicion of the diagnosis occurs if the right ventricle appears dilated, especially fatty, upon initial inspection of the heart (top left). Actually, aneurysms occur in approximately 35% of patients when evaluated by imaging. At autopsy, dilatation such as seen in this example occurs in 40-50% of cases, with true aneurysm being much less common. The fibrofatty involvement of the right ventricle (upper right) is typically patchy; in this case, a segment of fatty replacement exists, without significant thinning or aneurysm, features that were once considered pathognomonic of the disease. Left ventricular scarring is generally subepicardial, but in this case (bottom left), the scarring is more random, reflecting the phenotypic heterogeneity of ARVC. On cross-section (short axis cuts) seen at low magnification (bottom right), the changes are not particularly striking of a particular cardiomyopathy; it is almost the rule that careful examination for fibrofatty infiltrates is necessary for adequate sampling that will lead to diagnosis.
Microscopic Findings
Histologically, the ventricle appears randomly “moth-eaten,” with destruction of the normal myocytes via inflammation, scarring, and fat replacement. Inflammation is composed of lymphocytes and macrophages, with only rare myocyte necrosis. The myocytes in the involved areas appear attenuated, with loss of cross-striations and areas of myofibrillar loss imparting a “bubbly” appearance. The changes are nonspecific, as fat may be a component of ischemic scarring and myocyte vacuolization may be seen in other forms of cardiomyopathy, as well as inflammatory infiltrates. Diagnosis of arrhythmogenic right ventricular cardiomyopathy (ARVC) is generally made pathologically at autopsy. Endomyocardial biopsy is unreliable, as sampling the apical septum does not typically reveal diagnostic material.
Microscopic features of arrhythmogenic right ventricular cardiomyopathy (ARVC). These images are histologic sections from the heart illustrated in Media file 1. The top left demonstrates an area of fat in the right ventricle, with fibrous tissue highlighted by the Masson trichrome stain. The areas of fat are irregular, in contrast to the normal "marbling" appearance seen in the anterior right ventricle, in which relatively even linear fatty areas exist. The fat in ARVC is considered "metaplastic" or secondary to an area of prior myocyte destruction. In contrast to the right ventricle, the areas of involvement in the left ventricle (top right) are often less composed of fat, and more of fibrous tissue. A higher magnification demonstrates altered myocytes with vacuoles, which are seen in all areas of fibrofatty infiltration (bottom left). Depending on the degree of sampling and definition of myocarditis, inflammation with myocyte necrosis is seen in over 25% of cases (bottom right).
Immunohistochemistry
In general, immunohistochemistry is not useful in diagnosis. Some have recently postulated that diffuse loss of desmosomal proteins, as seen immunohistochemically, is suggestive of the diagnosis of arrhythmogenic right ventricular cardiomyopathy (ARVC). These proteins include connexin-43 and plakoglobin.11
Molecular/Genetics
Family studies have suggested that arrhythmogenic right ventricular cardiomyopathy (ARVC) is caused by genetic alterations in desmosomal proteins, especially plakoglobin and desmoplakin.12,13,14,15,16 A recent family study demonstrated desmosomal mutations in just fewer than 20% of patients.4
Prognosis and Predictive Factors
Because autopsy studies are skewed to fatal deaths, it has been assumed that arrhythmogenic right ventricular cardiomyopathy (ARVC) is uniformly lethal. The clinical diagnosis has been hampered by the nonspecificity of ECG and imaging findings. With improvements in cardiac MR and CT, the clinical diagnosis has become more precise.
Recent studies of families with ARVC have suggested that with antiarrhythmic treatment, including implantation of defibrillators, the prognosis may be improved. Young age, family history of juvenile sudden death, QRS dispersion greater than or equal to 40 ms, T-wave inversion, left ventricular involvement, ventricular tachycardia, syncope, and previous cardiac arrest are the major risk factors for adverse prognosis. Preparticipation screening for sport eligibility has been proven to be effective in detecting asymptomatic patients and sport disqualification has saved lives; sudden death in young athletes has substantially declined.1
Recent studies of families with ARVC have suggested that with antiarrhythmic treatment, including implantation of defibrillators, the prognosis may be improved. Young age, family history of juvenile sudden death, QRS dispersion greater than or equal to 40 ms, T-wave inversion, left ventricular involvement, ventricular tachycardia, syncope, and previous cardiac arrest are the major risk factors for adverse prognosis. Preparticipation screening for sport eligibility has been proven to be effective in detecting asymptomatic patients and sport disqualification has saved lives; sudden death in young athletes has substantially declined.1
Multimedia
 | Media file 1: Gross findings at autopsy, ventricular arrhythmogenic right ventricular cardiomyopathy (ARVC). A suspicion of the diagnosis occurs if the right ventricle appears dilated, especially fatty, upon initial inspection of the heart (top left). Actually, aneurysms occur in approximately 35% of patients when evaluated by imaging. At autopsy, dilatation such as seen in this example occurs in 40-50% of cases, with true aneurysm being much less common. The fibrofatty involvement of the right ventricle (upper right) is typically patchy; in this case, a segment of fatty replacement exists, without significant thinning or aneurysm, features that were once considered pathognomonic of the disease. Left ventricular scarring is generally subepicardial, but in this case (bottom left), the scarring is more random, reflecting the phenotypic heterogeneity of ARVC. On cross-section (short axis cuts) seen at low magnification (bottom right), the changes are not particularly striking of a particular cardiomyopathy; it is almost the rule that careful examination for fibrofatty infiltrates is necessary for adequate sampling that will lead to diagnosis. |
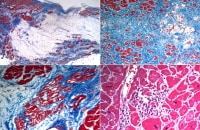 | Media file 2: Microscopic features of arrhythmogenic right ventricular cardiomyopathy (ARVC). These images are histologic sections from the heart illustrated in Media file 1. The top left demonstrates an area of fat in the right ventricle, with fibrous tissue highlighted by the Masson trichrome stain. The areas of fat are irregular, in contrast to the normal "marbling" appearance seen in the anterior right ventricle, in which relatively even linear fatty areas exist. The fat in ARVC is considered "metaplastic" or secondary to an area of prior myocyte destruction. In contrast to the right ventricle, the areas of involvement in the left ventricle (top right) are often less composed of fat, and more of fibrous tissue. A higher magnification demonstrates altered myocytes with vacuoles, which are seen in all areas of fibrofatty infiltration (bottom left). Depending on the degree of sampling and definition of myocarditis, inflammation with myocyte necrosis is seen in over 25% of cases (bottom right). |
 | Media file 3: Arrhythmogenic right ventricular cardiomyopathy (ARVC), biventricular, autopsy heart, young man who died suddenly playing basketball. Top left demonstrates increased fat in the outer walls of the right ventricle and left ventricular posterolateral walls. A higher magnification of the right ventricle is seen at top right; the anterior wall is nearly completely replaced with fat, and fibrofatty irregular posterior wall involvement is seen. Note that no actual thinning of the wall itself exists, although the muscular portion is in some areas completely missing. The bottom left demonstrates a full thickness of the right ventricle stained with Masson trichrome. The residual muscle is present only in a band-like area of scarring, and subepicardial scarring is present as well. The characteristic myocyte vacuolization, depicted at the bottom right, is seen in nearly all areas of ARVC within the scarred areas. |
Keywords
arrhythmogenic right ventricular cardiomyopathy-dysplasia, arrhythmogenic right ventricular cardiomyopathy, right ventricular dysplasia, left ventricular dysplasia, arrhythmogenic cardiomyopathy

0 comments:
Post a Comment