

Myelodysplastic Syndromes Associated With Isolated Del (5q)

Overview
Myelodysplastic syndrome (MDS) with isolated del(5q) is one of a group of clonal disorders of myeloid stem cells that are characterized by ineffective hematopoiesis, manifested in morphologic dysplasia of hematopoietic precursors and characterized by one or more peripheral blood cytopenias. In patients with MDS with isolated del(5q), the morphologic dysplasia is most evident as an increase in the number of small, hypolobated megakaryocytes. Patients typically present with marked macrocytic anemia and a normal or increased platelet count. Progression to acute myeloid leukemia (AML) is less common in MDS with isolated del(5q) than in other forms of MDS.
Disorders
Myelodysplastic syndrome associated with isolated del(5q)
Definition
MDS with isolated del(5q) is a myelodysplastic syndrome in which patients often present with macrocytic anemia with or without other cytopenias and normal to increased platelets in the peripheral blood. This form of MDS is defined in part by the presence of deletion in the long arm of chromosome 5 (del(5q)) as the sole cytogenetic abnormality. In cases of MDS with isolated del(5q), there are less than 5% blasts in the bone marrow and less than 1% blasts in the peripheral blood. In addition, Auer rods are not present.1
It should be noted that del(5q) is one of the most frequent abnormalities identified in MDS2 , including many cases of MDS associated with prior chemotherapy or with other cytogenetic abnormalities.3 In cases in which the patient has received prior chemotherapy, MDS in which del(5q) is the sole abnormality should be classified as a therapy-associated myelodysplastic syndrome (t-MDS). The prognosis for patients with t-MDS is not as favorable as the prognosis for patients with MDS with isolated del(5q). If additional cytogenetic abnormalities are present and the patient has no history of chemotherapy, the disease should be classified on the basis of morphologic parameters.
It should be noted that del(5q) is one of the most frequent abnormalities identified in MDS2 , including many cases of MDS associated with prior chemotherapy or with other cytogenetic abnormalities.3 In cases in which the patient has received prior chemotherapy, MDS in which del(5q) is the sole abnormality should be classified as a therapy-associated myelodysplastic syndrome (t-MDS). The prognosis for patients with t-MDS is not as favorable as the prognosis for patients with MDS with isolated del(5q). If additional cytogenetic abnormalities are present and the patient has no history of chemotherapy, the disease should be classified on the basis of morphologic parameters.
Epidemiology
Like other forms of MDS, MDS with isolated del(5q) is predominantly a disease of elderly persons; the median age of patients at the time of presentation is between 65 and 70 years. As described in van den Berghe's original series4 and as defined by the World Health Organization classification of tumors of hematopoietic and lymphoid tissues,1 MDS with isolated del(5q) is more common in women.
Clinical Features
In general, patients with MDS typically present with features associated with their cytopenia(s), such as fatigue, easy bleeding or bruising, or infection. Patients with MDS with isolated del(5q) typically present with persistent anemia that has no other identifiable cause. The neutrophil count is usually normal, and the number of platelets may be normal or even increased. The anemia often progresses to transfusion-dependence. Transformation to acute leukemia is uncommon in patients with this subtype of MDS, but patients sometimes succumb to complications related to transfusion-associated hemosiderosis.5
Until recently, there had been limited therapeutic options that were capable of altering the course of MDS. However, the use of lenalidomide, a thalidomide analogue, has improved outcomes in MDS patients, particularly those with del(5q). Its use leads to complete morphologic and cytogenetic remission in a significant number of cases.6
Until recently, there had been limited therapeutic options that were capable of altering the course of MDS. However, the use of lenalidomide, a thalidomide analogue, has improved outcomes in MDS patients, particularly those with del(5q). Its use leads to complete morphologic and cytogenetic remission in a significant number of cases.6
Morphologic Features
Patients with MDS with isolated del(5q) present with a striking macrocytic anemia and usually have normal or increased numbers of platelets in the peripheral blood. Leukocytopenia may be present; however, the number of granulocytes is typically normal. Bone marrow aspirates show predominantly megakaryocytic dysplasia with many small, hypolobated megakaryocytes (see Media files 1-3).
Normocellular bone marrow with increased numbers of small, hypolobated megakaryocytes. In this case, granulocytes and erythroid precursors show normal maturation (bone marrow aspirate, Wright-Giemsa, X1,000).
Small, hypolobated megakaryocytes are typical of myelodysplastic syndrome with isolated del(5q) (bone marrow aspirate, Wright-Giemsa, X1,000).
Normocellular bone marrow with trilineage hematopoiesis, including many megakaryocytes. Scattered hypolobated forms are present (bone marrow biopsy specimen, hematoxylin-eosin, X1,000).
Erythroid hypoplasia may be present. Erythroid and granulocytic dysplasia, if present, is generally mild. The bone marrow biopsy and clot sections generally show normocellular or mildly hypercellular bone marrow with numerous small megakaryocytes, sometimes forming clusters.7 Although some early series included patients with blast counts greater than 5%,8 such cases are better classified as either refractory anemia with excess blasts (5-19% blasts) or acute leukemia (20% or more blasts).
Immunophenotypic Features and Methods
There are no specific immunophenotypic findings associated with MDS with isolated del(5q). Immunohistochemical studies that assess for the presence of CD61 or factor VIII on bone marrow core biopsy specimens or clot sections may reveal the small, hypolobated megakaryocytes associated with this disease. Immunohistochemical studies for CD34 should reveal that few (less than 5%) mononuclear cells are immunoreactive.
Flow cytometric analysis may be of value in establishing a diagnosis of MDS. However, its utility in specifically establishing a diagnosis of MDS with isolated del(5q) has not been demonstrated.
Flow cytometric analysis may be of value in establishing a diagnosis of MDS. However, its utility in specifically establishing a diagnosis of MDS with isolated del(5q) has not been demonstrated.
Molecular/Genetic Features and Methods
As the name implies, in cases of MDS with isolated del(5q), cytogenetic studies demonstrate a deletion of the long arm of chromosome 5 (del(5q)) as the sole cytogenetic abnormality. In patients with myelodysplasia, deletions of 5q show considerable heterogeneity. Several genes localized to the long arm of chromosome 5q influence hematopoiesis and could be involved in the pathogenesis of the syndrome. Research aimed at delineating the specific chromosomal bands or genes that give rise to this form of MDS (the so-called common deleted region) have narrowed the region involved to band 5q32-5q339 in the 5q- syndrome. A distinct region at 5q31 is frequently found to be deleted in patients who have del(5q) associated with other chromosomal abnormalities or who have previously undergone chemotherapy.6
A gene involving ribosome biogenesis, RPS14, has been implicated in the pathogenesis of this syndrome, although this defect alone may not be sufficient to fully account for the spectrum of clinical and pathologic changes seen in the disease.10 It is possible that the phenotype of MDS in patients with del(5q) is influenced by deletion of multiple genes in this chromosome region.11
A gene involving ribosome biogenesis, RPS14, has been implicated in the pathogenesis of this syndrome, although this defect alone may not be sufficient to fully account for the spectrum of clinical and pathologic changes seen in the disease.10 It is possible that the phenotype of MDS in patients with del(5q) is influenced by deletion of multiple genes in this chromosome region.11
Prognosis and Predictive Factors
For patients with MDS with isolated del(5q), prognoses vary widely. In those cases that fit the classic description of 5q- syndrome, the prognosis is favorable, with prolonged median survival and a lower rate of transformation to AML, as compared with other forms of MDS. The presence of granulocytic dysplasia has been shown to be an independent adverse prognostic factor.12
In addition, the use of the immunomodulatory drug lenalidomide (an analogue of thalidomide) has shown promise in the treatment of MDS, particularly MDS with del(5q).13 Benefits were seen in patients with del(5q) as the sole abnormality, as well as in patients with del(5q) in association with other cytogenetic abnormalities. In over half of the patients with MDS with del(5q) who were treated with lenalidomide, transfusion independence was achieved, and a subset of patients exhibited a complete cytogenetic response. For patients with forms of MDS other than MDS with del(5q), response rates were lower.14 Additional studies with longer follow-up are needed to determine how this treatment affects overall survival.
In addition, the use of the immunomodulatory drug lenalidomide (an analogue of thalidomide) has shown promise in the treatment of MDS, particularly MDS with del(5q).13 Benefits were seen in patients with del(5q) as the sole abnormality, as well as in patients with del(5q) in association with other cytogenetic abnormalities. In over half of the patients with MDS with del(5q) who were treated with lenalidomide, transfusion independence was achieved, and a subset of patients exhibited a complete cytogenetic response. For patients with forms of MDS other than MDS with del(5q), response rates were lower.14 Additional studies with longer follow-up are needed to determine how this treatment affects overall survival.
DIFFERENTIALS
Multimedia
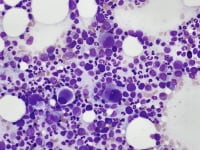 | Media file 1: Normocellular bone marrow with increased numbers of small, hypolobated megakaryocytes. In this case, granulocytes and erythroid precursors show normal maturation (bone marrow aspirate, Wright-Giemsa, X1,000). |
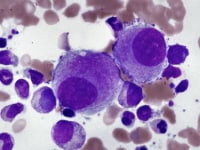 | Media file 2: Small, hypolobated megakaryocytes are typical of myelodysplastic syndrome with isolated del(5q) (bone marrow aspirate, Wright-Giemsa, X1,000). |
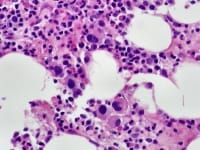 | Media file 3: Normocellular bone marrow with trilineage hematopoiesis, including many megakaryocytes. Scattered hypolobated forms are present (bone marrow biopsy specimen, hematoxylin-eosin, X1,000). |
Keywords
myelodysplastic syndromes associated with isolated del(5q), myelodysplastic syndrome, acute myeloid leukemia, MDS, AML, cytogenetic del(5q), 5q- syndrome

0 comments:
Post a Comment