

Cardiac Myxoma

Definition
The World Health Organization (WHO) defines a cardiac myxoma as a neoplasm composed of stellate to plump cytologically bland mesenchymal cells set in a myxoid stroma.1
Epidemiology
Epidemiological characteristics of cardiac myxomas are best divided into the following 2 categories: those that arise sporadically (95%) and those that occur in association with a so-called “myxoma syndrome” (5%).
Sporadic cardiac myxomas have been described in individuals as young as stillborn infants and as old as 97 years.2,3 Although they can be found anywhere in this very wide age range, sporadic cardiac myxomas are clearly more common among adults, who present at an average age of 50 years; furthermore, sporadic cardiac myxomas occur approximately twice as often in women as men.3,4
Sporadic cardiac myxomas have been described in individuals as young as stillborn infants and as old as 97 years.2,3 Although they can be found anywhere in this very wide age range, sporadic cardiac myxomas are clearly more common among adults, who present at an average age of 50 years; furthermore, sporadic cardiac myxomas occur approximately twice as often in women as men.3,4
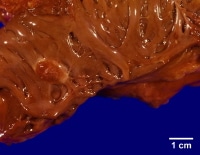
This gross photograph is an excellent example of a sessile myxoma arising within the left atrium. Note how the myxoma has a very broad attachment to the underlying myocardium.
Familial cardiac myxomas typically arise as part of the Carney complex (see Molecular/Genetics). Cardiac myxomas occurring in this setting arise in combination with 2 or more of the following lesions: skin myxomas, cutaneous lentiginosis, myxoid fibroadenomas of the breast, pituitary adenomas, and large-cell calcifying Sertoli-cell tumors of the testis.
Important demographic differences exist between the sporadic and familial cardiac myxomas. Familial cardiac myxomas appear to occur more commonly in men (2:1) and typically present in the third decade rather than the fifth decade.5
Important demographic differences exist between the sporadic and familial cardiac myxomas. Familial cardiac myxomas appear to occur more commonly in men (2:1) and typically present in the third decade rather than the fifth decade.5
Etiology
Although numerous theories have been posited regarding the etiology of cardiac myxomas, their precise histogenesis remains largely enigmatic. For a time, cardiac myxomas were believed to arise from mural thrombi.6However, the differences between myxomas and thrombi are substantial. Although mural thrombi tend to occur in individuals with underlying heart disease and in many locations within the heart (atrial appendages, atria, ventricles), myxomas arise with astonishing consistency in one location, primarily adjacent to the fossa ovalis.
Furthermore, histologically, myxomas do not organize into fibrous tissue or show stratification, a feature classic of mural thrombi. Cardiac myxomas also behave differently than thrombi in tissue culture studies.7 This body of evidence in support of the neoplastic nature of myxomas has led to the consensus that cardiac myxomas are not of thrombotic origin and are, indeed, neoplastic.8
The impetus for this neoplastic transformation is equally as unclear. Although genetics (see Molecular/Genetics) clearly plays a role in myxoma syndromes, genetics does not appear to offer a consistent explanation in sporadic cases. A recent study centers on the possibility of an infectious etiology. Li and colleagues recently reported finding evidence for HSV-1 infection in 70% of a relatively small cohort (n=17) of surgically resected, sporadic cardiac myxomas.
Regardless of the precise etiology of cardiac myxomas, the morphologic, ultrastructural, and immunoperoxidase studies done to date suggest that the neoplastic cells are of primitive multipotential mesenchymal origin.9,8,7
Furthermore, histologically, myxomas do not organize into fibrous tissue or show stratification, a feature classic of mural thrombi. Cardiac myxomas also behave differently than thrombi in tissue culture studies.7 This body of evidence in support of the neoplastic nature of myxomas has led to the consensus that cardiac myxomas are not of thrombotic origin and are, indeed, neoplastic.8
The impetus for this neoplastic transformation is equally as unclear. Although genetics (see Molecular/Genetics) clearly plays a role in myxoma syndromes, genetics does not appear to offer a consistent explanation in sporadic cases. A recent study centers on the possibility of an infectious etiology. Li and colleagues recently reported finding evidence for HSV-1 infection in 70% of a relatively small cohort (n=17) of surgically resected, sporadic cardiac myxomas.
Regardless of the precise etiology of cardiac myxomas, the morphologic, ultrastructural, and immunoperoxidase studies done to date suggest that the neoplastic cells are of primitive multipotential mesenchymal origin.9,8,7
Location
Most myxomas (75%) are located in the left atrium, with the remainder (18%) being found predominately in the right atrium.10 Equal incidence is found between the left and right ventricles (3% each), and only a very small fraction (<1%) involve the valves.11,12,13,14
These tumors are typically found arising from the region of the fossa ovalis. For a time, myxomas were thought to arise from minute endocardial endothelial structures known as “Prichard structures,” located primarily in the fossa ovalis.15 This theory has been largely discounted by recent studies that show no relation between the seemingly age-related Prichard structures and myxomas.16
Cardiac myxomas arising as part of the Carney complex occur somewhat less commonly in the left atrium (62%) and are often multicentric, occasionally involving multiple chambers.5
These tumors are typically found arising from the region of the fossa ovalis. For a time, myxomas were thought to arise from minute endocardial endothelial structures known as “Prichard structures,” located primarily in the fossa ovalis.15 This theory has been largely discounted by recent studies that show no relation between the seemingly age-related Prichard structures and myxomas.16
Cardiac myxomas arising as part of the Carney complex occur somewhat less commonly in the left atrium (62%) and are often multicentric, occasionally involving multiple chambers.5
Clinical Features
Cardiac myxomas elicit a wide variety of symptoms in patients, largely dependent on size and location of the tumor. Individuals with cardiac myxomas can present at any point along the clinical continuum, ranging from complete asymptomatology (particularly with tumors less than 40 mm in size) to sudden death, usually owing to acute obstruction or embolization.17,18
Although the clinical spectrum can be rather wide, most affected individuals present with one or more of a triad of symptoms (the so-called "myxoma triad"), which includes embolic phenomena, intracardiac flow obstruction, and constitutional symptoms.19,20,21,22 These symptoms, however, are rather nonspecific and often lead to a misdiagnosis owing to the relative rarity of myxomas (or cardiac tumors in general) that are encountered by most clinicians.23
Symptoms of intracardiac flow obstruction are the most commonly described manifestation, occurring in more than half of individuals with cardiac myxomas.1,24 Typically, these individuals show symptoms of left-sided heart failure (dyspnea, orthopnea, fatigue) or syncope. Likewise, right atrial myxomas can manifest with symptoms of right-sided heart failure (eg, systemic edema, hepatomegaly). Occasionally, a systolic or diastolic murmur can be auscultated. In some instances, the astute clinician may hear a characteristic “tumor plop” in early diastole.24
Somewhere on the order of 30-40% of individuals with cardiac myxomas experience embolic phenomena. Sites of embolization include the central nervous system, kidneys, extremities, and coronary arteries. The clinical manifestations of this embolization are broad and arise dependent upon the tissue downstream of the embolus. Note that paradoxical embolism may occur in individuals with an anatomically patent foramen ovale.25 Myxomas can also uncommonly serve as a nidus for infection.26 When this occurs, symptoms parallel those of infective endocarditis.
Nonspecific constitutional symptoms have been reported in anywhere from 20-60% of individuals with cardiac myxomas.1,10,24 These include such symptoms as fever, arthralgia, myalgia, and weight loss.21 Laboratory findings can include elevated erythrocyte sedimentation rate (33%), normochromic anemia (15%), and thrombocytopenia (5%). These findings are likely due to the tumor’s constitutive ability to elaborate interleukin (IL)-6, a cytokine that induces the acute-phase response. Individuals who experience these constitutional symptoms have been found to have higher serum levels of IL-6, with these levels dropping precipitously following removal of the tumor.27
Symptoms of intracardiac flow obstruction are the most commonly described manifestation, occurring in more than half of individuals with cardiac myxomas.1,24 Typically, these individuals show symptoms of left-sided heart failure (dyspnea, orthopnea, fatigue) or syncope. Likewise, right atrial myxomas can manifest with symptoms of right-sided heart failure (eg, systemic edema, hepatomegaly). Occasionally, a systolic or diastolic murmur can be auscultated. In some instances, the astute clinician may hear a characteristic “tumor plop” in early diastole.24
Somewhere on the order of 30-40% of individuals with cardiac myxomas experience embolic phenomena. Sites of embolization include the central nervous system, kidneys, extremities, and coronary arteries. The clinical manifestations of this embolization are broad and arise dependent upon the tissue downstream of the embolus. Note that paradoxical embolism may occur in individuals with an anatomically patent foramen ovale.25 Myxomas can also uncommonly serve as a nidus for infection.26 When this occurs, symptoms parallel those of infective endocarditis.
Nonspecific constitutional symptoms have been reported in anywhere from 20-60% of individuals with cardiac myxomas.1,10,24 These include such symptoms as fever, arthralgia, myalgia, and weight loss.21 Laboratory findings can include elevated erythrocyte sedimentation rate (33%), normochromic anemia (15%), and thrombocytopenia (5%). These findings are likely due to the tumor’s constitutive ability to elaborate interleukin (IL)-6, a cytokine that induces the acute-phase response. Individuals who experience these constitutional symptoms have been found to have higher serum levels of IL-6, with these levels dropping precipitously following removal of the tumor.27

0 comments:
Post a Comment