

Myocarditis

Myocarditis;
Definition
Myocarditis refers to an inflammatory response within the myocardium that is not secondary to ischemic events or cardiac rejection in the setting of transplantation. The presence of myocyte necrosis is required for certain types of myocarditis, specifically lymphocytic myocarditis that is triggered by viruses and augmented by autoimmunity, and the myocyte damage is believed to be mediated both by direct invasion of the myocardium and postimmune insult.
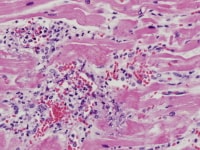
Lymphocytic myocarditis. Intermediate magnification of myocardium with diffuse infiltrates composed mostly of lymphocytes but also some neutrophils, macrophages, and plasma cells.
Histologically, some overlap exists among categories of myocarditis, and no finding is specific for a single etiology (see Microscopic Findings). In general, the histologic patterns can be divided into lymphocytic (including viral and autoimmune forms), eosinophilic (in which hypersensitivity myocarditis is the most common, followed by cases of hypereosinophilic syndrome), granulomatous (sarcoid and giant cell myocarditis [GCM]), neutrophilic (bacterial, fungal, and early forms of viral myocarditis), and reperfusion type/contraction band necrosis (present in catecholamine-induced injury and reperfusion injury). However, a pathologic classification is complicated because often tissue biopsies are not obtained and a presumptive clinical diagnosis is sometimes confirmed by indirect methods such as serology.
Epidemiology
The true incidence of myocarditis is difficult to determine, and most cases are believed to be subclinical. Laboratory tests are nonspecific, and endomyocardial biopsy is not performed in most cases. One study of military recruits that used ECG changes, clinical symptoms, and cardiac enzyme elevation estimated the incidence at 17 per 100,000 population annually.1,2
Less than 2% of all cases are fatal, and these are the cases that are commonly presented to pathologists. Fatal myocarditis cases often manifest as sudden or rapid death and have the highest incidence in infants and young adults. A slight male predominance is seen.
Etiology
Myocarditis cases usually fall into 4 main categories: infection, postviral autoimmune related, autoimmunity (lupus myocarditis, giant cell myocarditis [GCM]), and associated with drugs (hypersensitivity and toxic myocarditis). In over 50% of the cases, myocarditis is considered idiopathic and is believed to be postviral immune related, even in the absence of demonstrable viral antigens. Cases of viral myocarditis have an identifiable infectious organism ranging from 10-100% in several studies.3,4,5,6,7,8 Several factors influence the yield detection, including stage of the disease, the methods used to detect the infectious agent, sample studied (eg, heart from endomyocardial biopsy [EMB], autopsy material, or indirectly from serum), amount of available tissue, and interpretation of the results.
Myocarditis associated with drugs is histologically defined as hypersensitivity myocarditis. A list of medications associated with myocarditis includes clozapine, penicillin, ampicillin, hydrochlorothiazide, methyldopa, and sulfonamide drugs. Radiation therapy and insect bites are reported to cause heart injury as well. Toxic myocarditis relates to drug-induced injury that is not mediated by hypersensitivity and persists after the cessation of the drug. It is also associated with later inflammatory stages of catecholamine-induced myocardial injury.
Myocarditis associated with connective tissue disease has been reported in lupus, mixed connective tissue disease, rheumatoid arthritis, and others. Giant cell myocarditis [GCM] is considered idiopathic.
Location
Myocarditis most often refers to diffuse inflammation of the myocardium, although cases of focal myocarditis in either right or left ventricle have been reported. Cases of sudden death due to myocarditis show a diffuse infiltrate in all sections examined. However, areas of normal heart can be seen; this may explain the low sensitivity rate of endomyocardial biopsies.
Clinical Features
Patients with myocarditis may be asymptomatic, have very mild nonspecific symptoms, such as fever, chills, and dyspnea, or more severe symptoms like palpitations, syncope, and sudden death.
Most cases of myocarditis are acute self-limiting cases. Those patients typically have EKG alterations, cardiac enzymes elevation and some evidence of systemic inflammatory process (arthralgias, malaise, pharyngitis, tonsillitis, and upper respiratory tract infections). In these cases, infectious is the most common cause, viral infections being by far the most prevalent. Associated pericarditis is common. Most often, no indication for endomyocardial biopsy (EMB) exists, and the diagnosis is assigned clinically.
Some cases follow a rapid deterioration and have been named acute fulminant myocarditis. Fever is common. The presentation is acute with rapid onset of heart failure that may cause sudden death. The involvement of the myocardium is often diffuse, yielding a high sensitivity in EMB. In these cases, the histologic findings are usually lymphocytic, with a minor proportion showing eosinophilia typical of hypersensitivity myocarditis. Giant cell myocarditis (GCM) also occurs in rapid cases. Overall, these patients also have a good prognosis if early immunosuppression therapy is introduced. Antiviral agents do not seem to be of any value, because, in most cases, the viruses had been cleared from the organism.
A third scenario that is uncommon is that of chronic evolution to cardiomyopathy. These patients have a low detection of inflammation by EMB. The prognosis is poor, with some cases requiring heart transplantation.
Incidental myocarditis seen at autopsy that shows a focal lymphocytic process is another common situation. In these cases, lymphocytic myocarditis is again the most frequent finding, but hypersensitivity myocarditis is also common.
Gross Findings
The gross findings of fatal myocarditis cases are nonspecific and include normal or chamber dilatation. Softening and pallor of the ventricles can be present. Accompanied pericardial effusion and pericarditis can be part of viral or bacterial myocarditis cases. Late stages of myocarditis can show fibrosis that can be focal or diffuse, but the distribution is often random, as opposed to the subendocardial fibrosis typically seen in ischemia.
Myocarditis with scarring, autopsy. The image is a short axis gross photograph of an 8-year-old child with clinical myocarditis showing scarring of both ventricles, more prominent in the left. The fibrosis shows a random distribution with epicardial, myocardium, and pericardial involvements.
Microscopic Findings
Endomyocardial biopsy is generally indicated if heart failure exists; therefore, most suspected cases of myocarditis are not biopsied. Biopsy may be warranted when giant cell myocarditis (GCM) is suspected, to exclude sarcoidosis, in addition to unexplained recent onset of heart failure. The rate of myocarditis in biopsies for new onset of heart failure has been reported between 5% and 15%;9,10 although, according to one study, 12% of patients with new onset heart failure were given a clinical diagnosis of myocarditis.11
Endomyocardial biopsy of a 4-year-old child with clinical suspicion for myocarditis. This image is a low magnification of myocardium with lymphocytic infiltrate within myocardial fibers. The histologic findings are consistent with myocarditis and compatible with the clinical history, even in the absence of myocyte necrosis.
Immunohistochemical stained section of the biopsy illustrated in the prior figure showing positivity for CD3 confirming a T-cell phenotype.
The Dallas criteria for the biopsy diagnosis of myocarditis, established in 1987, consist of myocyte necrosis and inflammation. A positive biopsy, however, does not correlate with clinical symptoms; for example, fulminant from chronic myocarditis, which is diagnosed clinically and may respond to immunosuppressive therapy, may show only minimal inflammation because of sampling. The Dallas criteria include a “borderline” category for the first biopsy and “resolving myocarditis” for subsequent ones with no necrosis.12 Currently, any chronic inflammation in heart biopsy for new onset heart failure is diagnostic of myocarditis.
Lymphocytic myocarditis as seen at autopsy is rich in T cells and macrophages, and the inflammation is usually diffuse, with focal myocyte necrosis. In early phases of viral myocarditis, a neutrophilic infiltrate can occur and not be mistaken for bacterial etiology. The latter often shows numerous neutrophils, lymphocytes, and macrophages with prominent necrosis and occasional microabscesses, which are prominent in cases of fungal myocarditis. Inflammation due to ischemia is a major differential diagnosis at autopsy, especially at the edge of reperfusion infarcts, where a diffuse interstitial neutrophilic infiltrate may be present. Subendocardial location, a large proportion of neutrophils, extensive necrosis in relation to inflammation, and zonal necrosis in the case of nonreperfusion infarcts are features of ischemia.
Lymphocytic myocarditis as seen at autopsy is rich in T cells and macrophages, and the inflammation is usually diffuse, with focal myocyte necrosis. In early phases of viral myocarditis, a neutrophilic infiltrate can occur and not be mistaken for bacterial etiology. The latter often shows numerous neutrophils, lymphocytes, and macrophages with prominent necrosis and occasional microabscesses, which are prominent in cases of fungal myocarditis. Inflammation due to ischemia is a major differential diagnosis at autopsy, especially at the edge of reperfusion infarcts, where a diffuse interstitial neutrophilic infiltrate may be present. Subendocardial location, a large proportion of neutrophils, extensive necrosis in relation to inflammation, and zonal necrosis in the case of nonreperfusion infarcts are features of ischemia.
Lymphocytic myocarditis. Intermediate magnification of myocardium with diffuse infiltrates composed mostly of lymphocytes but also some neutrophils, macrophages, and plasma cells.
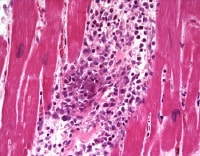
Focal lymphocytic myocarditis; intermediate magnification of myocardium with focal lymphocyte-rich infiltrate. Compare this with the diffuse process in Media file 1. The significance of focal inflammation at autopsy is often unclear, as such focal lesions can be found incidentally.
Lymphocytic myocarditis; high magnification of myocardium showing myocyte necrosis with lymphohistiocytic infiltrates.
Medium magnification of fungal myocarditis showing nonseptate hyphae within myocardium capillaries in association with lymphocytes and neutrophils.
The presence of giant cells and granulomas brings the differential diagnosis of giant cell myocarditis and sarcoid involving the heart. Some authors have used the term “granulomatous myocarditis” to illustrate any case with giant cells, such as in giant cell myocarditis and sarcoid. The cardiac findings of sarcoidosis are similar to other organs. The diagnosis is established by the presence of epithelioid granulomas with giant cell formation and associated with a variety of inflammatory cells consisting of activated T lymphocytes with increased CD4/CD8 ratios and activated monocytes and macrophages.
Giant cell myocarditis is characterized by diffuse infiltration of myocardium by a heterogeneous infiltrate composed of abundant lymphocytes, some eosinophils and plasma cells, occasional neutrophils and scattered prominent giant cells. T lymphocytes are more numerous than B cells, with a predominance of CD8 T lymphocytes. Myocyte degenerative changes and myocyte necrosis, especially in early stages of the disease, are invariably present. Contrasted with CS, in GCM the giant cells are not part of well-formed granulomas, are associated with myocyte necrosis, and do not involve the interstitium and epicardium. Eosinophils can be easily found in GCM, and they are rare in CS.13
Giant cell myocarditis; intermediate magnification in a sudden death case. Diffuse with numerous giant cells, lymphocytes, neutrophils, and eosinophils is present. Myocyte damage is also present.
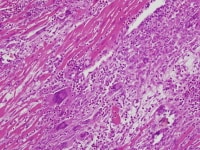
Cardiac sarcoidosis; low magnification of autopsy case with numerous giant cells and lymphocytes in a background of fibrosis and scarring. In addition to the cardiac findings, this patient had extensive involvement of mediastinal lymph nodes by sarcoidosis.
Eosinophilic myocarditis is usually related to hypersensitivity myocarditis and is described as infiltrates rich in macrophages and eosinophils. In this setting, myocyte necrosis is usually not present, and scattered poorly formed granulomas can be seen. This histologic pattern is more frequent as incidental findings in explants from heart transplant candidates, or at autopsy, with no history of any symptoms. The differential diagnosis is eosinophilic endomyocardial disease (Loeffler syndrome), which is characterized by extensive necrosis and mural and intravascular thrombi and is not considered myocarditis in either clinical or pathological settings. Rarely, hypersensitivity myocarditis can result in myocyte damage and severe clinical symptoms; this condition is important to diagnose by biopsy because cardiac function may improve or normalize when the offending drug is withheld.
Hypersensitivity myocarditis; high magnification of myocardium with perivascular infiltrates rich in eosinophils. This patient had a clinical history compatible with drug-induced hypersensitivity myocarditis.
Immunohistochemistry
The inflammatory cells are most frequently mature T-lymphocytes with a large population of accompanying macrophages. The T-cells are a mixture of CD4+ and CD8+ cells. Immunohistochemical and in-situ hybridization assays are available for the identification of a multitude of microorganisms that comprise viruses, bacteria, and parasites (including T gondii and T cruzi).8 Several studies have documented the use of PCR in EMB and autopsy tissue in the detection of parvovirus, adenovirus, enterovirus (most often coxsackievirus), Epstein-Barr virus, Lyme borreliosis, and others.4,8,14,15,16,17
However, other studies have also shown the presence of organisms when cardiac tissue lacks evidence of inflammation, raising questions about the specificity of the detection and reinforcing the need for clinic-pathological correlation and accurate histologic diagnosis of myocarditis.18,19
However, other studies have also shown the presence of organisms when cardiac tissue lacks evidence of inflammation, raising questions about the specificity of the detection and reinforcing the need for clinic-pathological correlation and accurate histologic diagnosis of myocarditis.18,19
Molecular/Genetics
Great interest has recently arisen on the finding of etiologic microbiologic agents in cases of myocarditis using endomyocardial biopsy or autopsy material. However, the identification of organisms, especially viruses, in clinical samples is problematic because of a high range of reported positivity. Polymerase chain reaction has been used to detect viruses and other pathogens in biopsy and autopsy samples of myocarditis and cardiomyopathy PCR in EMB and autopsy, including parvovirus, adenovirus, enterovirus (most often coxsackievirus), Epstein-Barr virus, and Lyme borreliosis.7,16,18 However, positive PCR results in control tissues hamper interpretation of the findings.19,20
Prognosis and Predictive Factors
Most cases of lymphocytic myocarditis are subclinical and never present to medical attention. Most patients resolve spontaneously with no known sequela. As stated above, a small percentage of patients, mostly children and young adults, present as fulminant disease onset and may progress rapidly to sudden death. In these patients, the infiltrates are usually diffuse. Another subset of patients who develop congestive heart failure may have late morbidity related to the degree of left ventricular dysfunction. Cases of giant cell myocarditis are usually severe, with a higher percentage progressing to death in a short period of time. Heart transplantation in association with immunosuppressive therapy is one of the only ways of saving most of these patients
Patients with hypersensitivity myocarditis and heart failure can improve and heal if the drug is discontinued, but some patients may require heart transplantation. More frequently, the pathologist sees incidental hypersensitivity at autopsy or explant that is asymptomatic. For example, in heart transplant patients, who are often on multiple medications, the incidence is 7%, as diagnosed histologically in the explanted heart.20
Differentials
Cardiac lymphoma
Heart Transplantation
Heart transplantation rejection
Inflammation induced by ischemia
Heart Transplantation
Heart transplantation rejection
Inflammation induced by ischemia
Multimedia
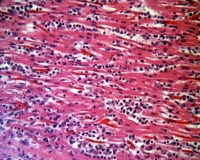 | Media file 1: Lymphocytic myocarditis. Intermediate magnification of myocardium with diffuse infiltrates composed mostly of lymphocytes but also some neutrophils, macrophages, and plasma cells. |
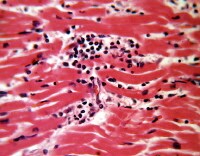 | Media file 2: Focal lymphocytic myocarditis; intermediate magnification of myocardium with focal lymphocyte-rich infiltrate. Compare this with the diffuse process in Media file 1. The significance of focal inflammation at autopsy is often unclear, as such focal lesions can be found incidentally. |
 | Media file 3: Giant cell myocarditis; intermediate magnification in a sudden death case. Diffuse with numerous giant cells, lymphocytes, neutrophils, and eosinophils is present. Myocyte damage is also present. |
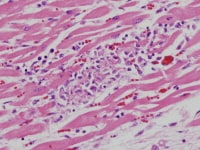 | Media file 4: Lymphocytic myocarditis; high magnification of myocardium showing myocyte necrosis with lymphohistiocytic infiltrates. |
 | Media file 5: Medium magnification of fungal myocarditis showing nonseptate hyphae within myocardium capillaries in association with lymphocytes and neutrophils. |
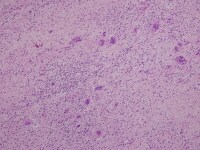 | Media file 6: Cardiac sarcoidosis; low magnification of autopsy case with numerous giant cells and lymphocytes in a background of fibrosis and scarring. In addition to the cardiac findings, this patient had extensive involvement of mediastinal lymph nodes by sarcoidosis. |
 | Media file 7: Hypersensitivity myocarditis; high magnification of myocardium with perivascular infiltrates rich in eosinophils. This patient had a clinical history compatible with drug-induced hypersensitivity myocarditis. |
 | Media file 8: Myocarditis with scarring, autopsy. The image is a short axis gross photograph of an 8-year-old child with clinical myocarditis showing scarring of both ventricles, more prominent in the left. The fibrosis shows a random distribution with epicardial, myocardium, and pericardial involvements. |
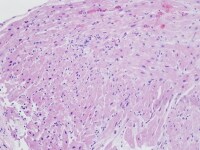 | Media file 9: Endomyocardial biopsy of a 4-year-old child with clinical suspicion for myocarditis. This image is a low magnification of myocardium with lymphocytic infiltrate within myocardial fibers. The histologic findings are consistent with myocarditis and compatible with the clinical history, even in the absence of myocyte necrosis. |
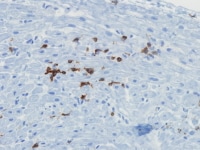 | Media file 10: Immunohistochemical stained section of the biopsy illustrated in the prior figure showing positivity for CD3 confirming a T-cell phenotype. |
Keywords
myocarditis, lymphocytic myocarditis, sarcoid, giant cell myocarditis, toxic myocarditis, reperfusion injury, granulomatous myocarditis, myocarditis symptoms, acute myocarditis, chronic myocarditis, myocarditis pathology

0 comments:
Post a Comment