

Pleomorphic Adenoma
_parotid_gland.jpg)
Pleomorphic AdenomaPleomorphic adenoma is a benign salivary gland tumor with wide cytomorphologic and architectural diversity. The tumor has 3 components: an epithelial cell component; a myoepithelial cell component; and a stromal (mesenchymal) component. The identification of these 3 components, which may vary quantitatively from one tumor to another, is essential to the recognition of pleomorphic adenoma. The tumor is also known as a benign mixed tumor.
Epidemiology
Pleomorphic adenoma is the most common salivary gland tumor in both children and adults. In most series, it represents 45-75% of all salivary gland neoplasms1,2 ; the annual incidence is approximately 2-3.5 cases per 100,000 people.3
Pleomorphic adenoma is more often seen in females than in males (2:1 ratio).
Pleomorphic adenoma occurs in individuals of all ages. It occurs most commonly in the third to sixth decades; the average age at presentation is from 43-46 years.4
Etiology
The etiology of pleomorphic adenoma is unknown; however, it has been noted that the incidence increases 15-20 years after exposure to radiation.1 One study suggests that the simian virus (SV40) may play an etiologic role in the development of pleomorphic adenoma.5
Location
Among the major salivary glands, the tail of the superficial lobe of the parotid salivary gland is the most common site of occurrence (70-80%), although it can occur in any parotid location. It is less commonly seen in the submandibular salivary gland (10%) and is seldom encountered in the sublingual gland (1%).6,7 In minor salivary glands (5-10%), the palate (specifically, the junction of the soft and hard palates) and the lip are the most common sites. Other sites of minor salivary gland involvement include the nose, the paranasal sinuses, and the larynx.
Rare or unusual sites of occurrence include ectopic salivary gland tissues (eg, mandible, neck lymph nodes, axilla).
Multiple tumors are unusual (1:40,000), but metachronous and synchronous tumors do occur.8,9,10,11Synchronous occurrence of pleomorphic adenoma and Warthin’s tumor (the second most common benign salivary gland tumor) has been reported.12,13,14,15
Multiple tumors are unusual (1:40,000), but metachronous and synchronous tumors do occur.8,9,10,11Synchronous occurrence of pleomorphic adenoma and Warthin’s tumor (the second most common benign salivary gland tumor) has been reported.12,13,14,15
Clinical Features and Imaging
Pleomorphic adenoma usually presents as a slow growing, painless mass; the mass may be present for many years.
Symptoms and signs depend on the location.7 When the tumor occurs in the parotid gland, signs of facial nerve weakness are seldom encountered; in large neglected tumors, facial nerve weakness is likely to arise as the result of malignant change. Pleomorphic adenoma in the deep lobe of the parotid gland may present as an oral retrotonsillar mass/parapharyngeal space tumor; indeed, tumors arising in the deep lobe of the parotid gland are the source of the most common parapharyngeal space tumors. A rapid enlargement of a tumor nodule should raise concern about the development of malignant change.
Patients with minor salivary gland tumors may present with a variety of symptoms, depending on the site of the tumor; such symptoms include dysphagia, dyspnea, hoarseness, difficulty chewing, and epistaxis.
Patients with minor salivary gland tumors may present with a variety of symptoms, depending on the site of the tumor; such symptoms include dysphagia, dyspnea, hoarseness, difficulty chewing, and epistaxis.
Gross Findings
Pleomorphic adenoma is a single, firm, mobile, well-circumscribed mass. The tumor may be whitish-tan to gray to bluish in color. In size, pleomorphic adenomas may vary from a few millimeters to large or even giant.16,17 They are irregularly shaped and have a bosselated surface.
Degenerative and cystic changes may be seen on sectioning. It is not unusual to observe evidence of focal or massive infraction. Recurrent tumors characteristically tend to present as multiple nodules of variable size.
Degenerative and cystic changes may be seen on sectioning. It is not unusual to observe evidence of focal or massive infraction. Recurrent tumors characteristically tend to present as multiple nodules of variable size.
Microscopic Findings
In the parotid gland, the tumor is usually surrounded by a fibrous capsule of variable thickness that may be focally deficient, especially in more mucoid tumors (see Media file 1). In minor salivary glands, no capsule is usually seen. Microscopic satellite tumor nodules, pseudopodia, and capsular penetration may be seen beyond the capsule (see Media file 5). This may be the cause of recurrence of pleomorphic adenomas in cases treated with simple enucleation or in cases in which surgical resection was performed with inadequate surgical margins.18,19,20
Capsule in pleomorphic adenoma. Image A shows a pleomorphic adenoma with a thin fibrous capsule separating the tumor from the surrounding normal parotid gland tissue. Image B shows a pleomorphic adenoma with a less well-developed focally absent capsule. Note the small satellite tumor nodule (arrow) protruding outside the major tumor mass.
Recurrence of pleomorphic adenoma. This image shows a recurrent pleomorphic adenoma with two microscopically benign–appearing nodules. A multinodular tumor pattern is characteristic in recurrent pleomorphic adenomas.
The epithelial component consists of epithelial and myoepithelial cells with divergent growth patterns, including trabecular, tubular, solid, cystic, and papillary architecture (see Media file 3). Pure epithelial cells are mainly cuboidal. Cells that exhibit myoepithelial features21,22 may have plasmacytoid, epithelioid, spindle, oncocytic, or clear cell morphology. In some studies, the most common myoepithelial cell type that was encountered displayed plasmacytoid cell morphology; the spindle cell type was the next most common type.23 All cellular elements appear cytologically bland, with no significant mitotic activity.
Cells in pleomorphic adenoma. Image A shows tubule/duct formations in pleomorphic adenoma. A well-defined inner epithelial lining, consisting of cuboidal cells with eosinophilic cytoplasm, which can focally be clear, is surrounded by a collar of one or more layers of myoepithelial cells with mostly clear cytoplasm. The stroma in between contains dispersed spindled and epithelioid myoepithelial cells. In image B, a similar tubular arrangement is seen, but the collar of myoepithelial cells is not as well defined. The stroma in between shows dispersed spindled myoepithelial cells. In both images note the bland nature of cells and the absence of atypia.
The ducts and tubules seen in pleomorphic adenomas usually exhibit a double-cell– type lining—that is, an inner cuboidal epithelial cell layer and an outer myoepithelial cell layer (or layers) tend to merge into the surrounding stromal component, which also contains dispersed or grouped modified myoepithelial cells. The cuboidal epithelial cells occasionally have a clear cytoplasm; the myoepithelial cell cytoplasm varies from being deeply eosinophilic to clear. In a limited biopsy specimen or in fine-needle aspiration, the characteristics seen in the ductal or tubular elements may cause the pleomorphic adenoma to be confused with other salivary gland tumors exhibiting a similar architecture, such as adenoid cystic carcinoma and epithelial-myoepithelial carcinoma. In some cases, the tubules or ducts have a less well-defined surrounding myoepithelial layer.
The stromal component is a product of the modified myoepithelial cells and may appear mucoid, myxoid, hyaline, chondroid, myxochondroid, or even osseous (see Media file 2).24,25 The stromal modified myoepithelial cell may undergo chondroid or osseous metaplasia.26 Chondroid areas represent true cartilage formation (containing type II collagen and keratin sulphate); such a finding tends to be specific to pleomorphic adenoma—a fact that helps in differentiating pleomorphic adenoma from other suspected salivary gland tumors.
A prominent hyalinized stroma has been found by some authors to correlate with ancient tumors and tumors that may have a propensity for malignant change.27 It is important to note that other salivary gland tumors may exhibit exuberant hyalinization; chief among these is adenoid cystic carcinoma.
A prominent hyalinized stroma has been found by some authors to correlate with ancient tumors and tumors that may have a propensity for malignant change.27 It is important to note that other salivary gland tumors may exhibit exuberant hyalinization; chief among these is adenoid cystic carcinoma.
Different types of stroma in pleomorphic adenoma. Image A shows a myxoid stroma. Note the dispersed spindle myoepithelial cells in the stroma, some of which have a stellate morphology. Image B shows a chondroid stroma. Image C shows stroma with cartilage formation. Image D shows a hyalinized stroma.
In cases in which the cellular elements predominate, the result is an epithelial cell- and/or myoepithelial-cell–rich or cellular pleomorphic adenoma; in cases in which the mesenchymal/stromal component predominates, the result is a stroma-rich pleomorphic adenoma (see Media file 4). A pleomorphic adenoma with an equal proportion of both components is often referred to as classic or mixed type. No clinical difference in behavior is seen as a result of these different cellular/stromal proportions.1 In many cases, however, different regions in the same tumor show striking variation in morphology and cellularity.
Cellularity in pleomorphic adenoma. This image shows a tumor with two contrasting regions. Visible in the right upper part of the image is a cellular region with a dense epithelial and myoepithelial cell component. In the left lower part of the image, the dominant morphology is that of a chondroid stroma, with only a few interspersed myoepithelial cells.
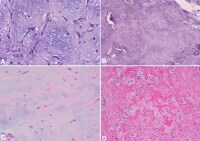
Pleomorphic adenoma occasionally exhibits unusual components, including sebaceous cells, mucous cells, squamous cells, oncocytic cells,28 serous acini, fibroadipose tissue,29 and crystal formations such as tyrosine or oxalate crystals (see Media file 6). The presence of mucous cells in pleomorphic adenoma, particularly in limited biopsy specimens, may prompt the examiner to consider entities such as mucoepidermoid carcinoma.30,31However, the presence of other components (eg, stroma, myoepithelial cells) helps establish the correct interpretation.
Unusual findings in pleomorphic adenoma. Image A shows tyrosine crystals with characteristic rosette appearance. Image B shows large cystic changes in a pleomorphic adenoma that is rich in myoepithelial cells. The arrow indicates an area of squamous cell metaplasia. Image C shows foci of mature adipose tissue (fat) in the stroma. Note the myoepithelial-rich stroma in the background. In Image D, areas of mucous signet–appearing cells (arrows) are present next to epithelial/myoepithelial formations.
Cystic changes are occasionally seen in pleomorphic adenoma—a large cyst may be present, or the tumor may be multicystic. However, such changes do not have an impact on the clinical course of the tumor.
Necrosis and increased mitosis are not commonly encountered in pleomorphic adenoma; when they do occur, a thorough search for evidence of malignant change is necessary. Fine-needle aspiration or focal infarction may result in similar tumor changes, and this should also be carefully considered. Other atypical findings, such as increased cellularity, focal atypia, pleomorphism, and capsular extension, should not be interpreted as being indicative of malignant change in the absence of other corroborating evidence. The occasional presence of benign tumor fragments within vascular spaces in the tumor or in the immediate peritumoral vasculature is thought to result from perioperative manipulation of the tumor during surgical resection and should not be interpreted as an indication of vascular invasion.25
Immunohistochemistry
In most instances, the diagnosis of pleomorphic adenoma is a straightforward microscopic identification. However, immunohistochemistry may be supportive and helpful in delineating the different cell types and components, as well as in differentiating pleomorphic adenoma from other tumors.32,33,34,35
The following immunohistochemical stains have proven to be helpful.
- Keratin - Positive in luminal epithelial and abluminal basal/myoepithelial cells
- Cam 5.2 and EMA - Positive in luminal epithelial cells
- P-63 - Positive in abluminal basal and myoepithelial cells
- Calponin, maspin, S-100 - Positive in myoepithelial cells
- HHF-35 - Smooth muscle myosin
- Muscle-specific actin - Positive in myoepithelial cells
- Glial fibrillary acidic protein - Positive in myoepithelial cells in myxoid areas
- BMP - Positive in myoepithelial cells in myxoid and chondroid areas
- BMP-6 - Positive in the cells in cartilage and in inner ductal cells
- Aggrecan - Positive in myxochondroid matrix
Molecular/Genetics
Most cases of pleomorphic adenomas (70%) show cytogenetic aberrations36,2,37,38,39,40,41 that manifest themselves in 3 patterns, as follows:
- Rearrangement of chromosome band 8q12 (target gene is PLGA1) in 39% of cases
- Rearrangement of chromosome band 12q13-15 (target gene is the high mobility group protein gene, HMGA2) in 8% of cases
- Sporadic or clonal changes not involving the above two chromosomes in 23% of cases
Both PLGA1 and HMGA2 gene translocations have been identified as tumor specific in pleomorphic adenoma; their detection by real-time polymerase chain reaction (RT-PCR) or fluorescence in situ hybridization aids in establishing a diagnosis of pleomorphic adenoma.
Interestingly, recent findings demonstrated the simian virus (SV40) sequence in human pleomorphic adenoma, suggesting an etiologic link.5
Interestingly, recent findings demonstrated the simian virus (SV40) sequence in human pleomorphic adenoma, suggesting an etiologic link.5
Prognosis and Predictive Factors
In most cases, the prognosis of patients with benign, well-circumscribed tumors tends to be excellent following surgical resection. However, recurrence can be a problem with pleomorphic adenomas, particularly those occurring in the parotid gland.42 Recurrence has been related to many factors, including an incomplete capsule, extension of tumor nodules beyond the capsule, and intraoperative tumor rupture, in which tumor contents spill into the operative field. Recurrence usually occurs in a multinodular fashion.43,44 In some cases, recurrence involves microscopic elements, rendering operative control extremely difficult and increasing the risk of multiple further recurrences, as well as the risk of future malignant transformation. Recurrences have been related to tumors with high mesenchymal content, particularly chondroid and myxoid stroma. Interestingly, in some series, recurrences seem to be more common in younger patients than in theolder ones.45A pleomorphic adenoma may undergo a malignant change that is not fully appreciated, owing to the fact that the malignant tumor is well-differentiated and has a bland cellular morphology at a level indistinguishable from the benign counterpart, particularly with small biopsy specimens or fine-needle aspirations. In such cases, a malignant recurrence may be erroneously presumed to be benign. One example of this that is becoming increasingly recognized in the literature is a well-differentiated myoepithelial carcinoma ex pleomorphic adenoma with mild cytologic atypia that is presumed to be a cellular pleomorphic adenoma. In these cases, the malignant change can be recognized only after careful assessment of the resected specimen and the discovery of evidence of malignancy (which is sometimes subtle).46
Malignant change occurs in 2-7% of cases and shows some association with multiple recurrences, deep lobe tumors, male gender, and older age.
Differentials
| Adenoid cystic carcinoma | Myoepithelioma |
| Adnexal neoplasms | Soft-tissue tumors (eg, soft-tissue tumors with myxoid change, as occurs in myxoid neurofibroma and myxomas) |
| Epithelial-myoepithelial carcinoma | |
| Low-grade polymorphous adenocarcinoma | |
| Mucoepidermoid carcinoma |
Multimedia
 | Media file 1: Capsule in pleomorphic adenoma. Image A shows a pleomorphic adenoma with a thin fibrous capsule separating the tumor from the surrounding normal parotid gland tissue. Image B shows a pleomorphic adenoma with a less well-developed focally absent capsule. Note the small satellite tumor nodule (arrow) protruding outside the major tumor mass. |
 | Media file 2: Different types of stroma in pleomorphic adenoma. Image A shows a myxoid stroma. Note the dispersed spindle myoepithelial cells in the stroma, some of which have a stellate morphology. Image B shows a chondroid stroma. Image C shows stroma with cartilage formation. Image D shows a hyalinized stroma. |
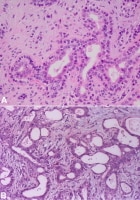 | Media file 3: Cells in pleomorphic adenoma. Image A shows tubule/duct formations in pleomorphic adenoma. A well-defined inner epithelial lining, consisting of cuboidal cells with eosinophilic cytoplasm, which can focally be clear, is surrounded by a collar of one or more layers of myoepithelial cells with mostly clear cytoplasm. The stroma in between contains dispersed spindled and epithelioid myoepithelial cells. In image B, a similar tubular arrangement is seen, but the collar of myoepithelial cells is not as well defined. The stroma in between shows dispersed spindled myoepithelial cells. In both images note the bland nature of cells and the absence of atypia. |
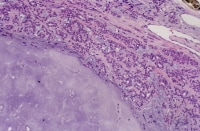 | Media file 4: Cellularity in pleomorphic adenoma. This image shows a tumor with two contrasting regions. Visible in the right upper part of the image is a cellular region with a dense epithelial and myoepithelial cell component. In the left lower part of the image, the dominant morphology is that of a chondroid stroma, with only a few interspersed myoepithelial cells. |
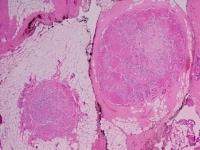 | Media file 5: Recurrence of pleomorphic adenoma. This image shows a recurrent pleomorphic adenoma with two microscopically benign–appearing nodules. A multinodular tumor pattern is characteristic in recurrent pleomorphic adenomas. |
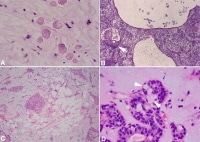 | Media file 6: Unusual findings in pleomorphic adenoma. Image A shows tyrosine crystals with characteristic rosette appearance. Image B shows large cystic changes in a pleomorphic adenoma that is rich in myoepithelial cells. The arrow indicates an area of squamous cell metaplasia. Image C shows foci of mature adipose tissue (fat) in the stroma. Note the myoepithelial-rich stroma in the background. In Image D, areas of mucous signet–appearing cells (arrows) are present next to epithelial/myoepithelial formations. |
Keywords
pleomorphic adenoma, benign mixed tumor, salivary gland benign mixed tumor

0 comments:
Post a Comment